Former NTSB and FAA investigator Jeff Guzzetti explains how seemingly small maintenance errors can lead to tragic circumstances, especially in helicopters.
System or component failures are among the most common defining events for fatal accidents in helicopters. Sadly, the circumstances of new accidents are often similar to those of previous ones, suggesting that some mechanics are not taking advantage of the lessons learned from such tragedies.
Five years ago, while working in FAA’s accident investigation division, I crossed paths with the investigations of two fatal accidents, occurring two months apart, and involving two Bell helicopters that were manufactured within a two-year period. In the end, both crashed due to improper maintenance and a lack of grease on a drive shaft. You can’t make this stuff up.
Pearl Harbor
The first crash occurred in Hawaii on the morning of February 18, 2016, when a Bell 206B, operated by Genesis Helicopters, was in the middle of a Part 91 air tour flight around the island of Oahu with four passengers on board. The 35-year-old commercial pilot and former Army Black Hawk driver noticed a vibration throughout the cabin, so he cut the tour short and diverted toward the destination airport.
The vibration developed into a grinding noise and was followed by the main rotor low rpm warning light and an increase in engine rpm. The pilot initiated an approach to a grassy area near the shoreline next to the Pearl Harbor Visitor Center. He noticed people near his intended landing area, so he altered his course to land in the water close to the shore. The helicopter impacted the water, rolled over, and began to sink (see graphic 1). A few shocked bystanders jumped in to pull the pilot and three of the four passengers out of the water. Unfortunately, a 15-year-old boy was trapped inside and drowned.
Shortly after my office received the notification, a video of the accident surfaced on social media and went viral (https://youtu.be/0sTTGlqZDx0). I considered dispatching one of our senior FAA investigators to the accident, but Hawaii was a long way away, and the Honolulu FAA Flight Standards office had a very capable inspector who was already at the scene and working with the National Transportation Safety Board (NTSB) investigator in charge. We decided to support the investigation from afar.
Genesis Helicopters operated only one helicopter under a Part 91 Letter of Authorization (LOA) from the FAA to conduct air tours within 25 statute miles of the departure airport. It employed only four people: the owner, the pilot, a receptionist, and a maintenance “assistant.” At the time, FAA policy stated that FAA should conduct inspections of 10% of all Part 91 air tour operators with an LOA, which could include ramp inspections, aircraft records review, or airworthiness directive compliance. The FAA inspector assigned to Genesis was interviewed by NTSB and stated that he had not completed a ramp inspection of the company since being assigned to it three months prior, but was trying to schedule a visit. Ironically, on the morning of the accident, he called the owner to schedule a records inspection but was unable to reach anyone.

Drive Shaft Separation
The pilot stated that he was descending to land when it felt like the main rotor stalled and the helicopter “fell out of the sky” about 20 feet from touchdown. The Bell 206B was built in 1979 and was powered by a single Allison 250-C20B turboshaft engine. It was removed from the water, rinsed with fresh water, and taken to a secure location for examination.
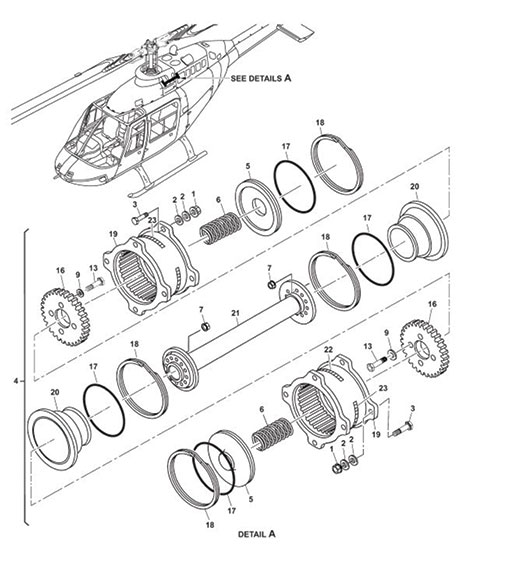
The wreckage exam showed no problems with the engine. However, the drive shaft section from the engine to the transmission was found separated at the transmission side (see graphics 2 and 3 previous page). Interviews with the accident pilot, the owner of the company, and the non-rated “maintenance assistant” revealed that maintenance had recently been conducted on the engine-to-transmission drive shaft, even though this work was not recorded in the helicopter’s maintenance records. In addition, the owner, who was a rated mechanic, was not present the entire time of the removal, inspection, and reinstallation of the drive shaft. To make matters worse, the maintenance records revealed no entries for a current annual or 100-hour inspection, and several required component inspections were overdue.

the drive shaft had failed.
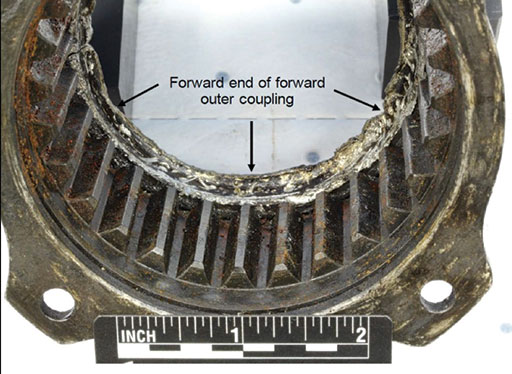
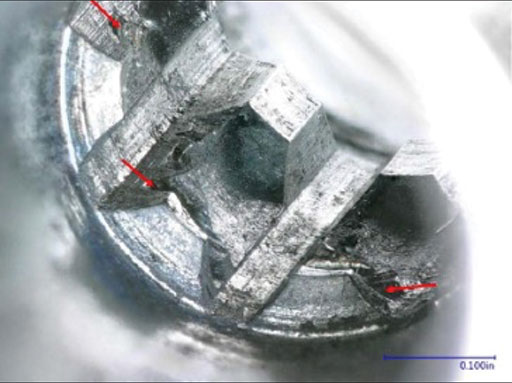
The drive shaft was sent to the NTSB Materials Lab in Washington, one block away from my office. The metallurgical exam revealed that the forward coupling of the drive shaft did not appear to be lubricated and had been exposed to high temperatures. The external spline teeth on the inner portion of the coupling were worn down to the bottom landings, while comparatively minor wear marks were observed on the mating teeth of the forward outer coupling (see graphics 4 and 5). The asymmetry in the wear pattern, combined with the observations of elevated temperatures, indicated that the assembly likely failed by overheating from a lack of lubrication. This resulted in softening and subsequent failure of the spring that centers the coupling. When the spring failed, the coupling shifted forward, damaging the forward end of the outer coupling, fracturing the forward cover plate, and wearing the external spline teeth down to the bottom landings. Following the failure of the drive shaft, the engine continued to operate, but was not able to drive the main rotor.
The NTSB opined that when maintenance was last conducted on the drive shaft, grease was not applied to the forward coupling as specified in the manufacturer’s maintenance manual. The NTSB probable cause was “the in-flight failure of the engine-to-transmission drive shaft due to improper maintenance, which resulted in low main rotor rpm and a subsequent hard landing to water.” The NTSB also cited numerous findings in the investigation, such as the operator’s failure to conduct scheduled and routine maintenance checks, and the lack of robust FAA requirements to oversee Part 91 air tour operations. That last finding troubled me, because the FAA would have likely caught the operator’s maintenance failures if it were required to operate under more stringent Part 135 commercial rules.
Great Smoky Mountains
Two months later, in April 2016, another Bell 206 helicopter was destroyed when it impacted terrain while maneuvering near Pigeon Forge, Tenn. Tragically, the 1,300-hour commercial pilot and all four passengers were killed. Just prior to the accident, a ground witness observed the helicopter at a low altitude in a descent and noted that it sounded unusual. He then heard the engine go silent, followed by the sound of the impact. The helicopter was operated by Great Smoky Mountain Helicopters, another small Part 91 air tour operator with a fleet of two ships (see graphic 6). The accident ship was built in 1977, two years before the birth of the Hawaii helicopter that had just crashed.

We now had two helicopters, built two years apart, and crashing two months apart, each during Part 91 air tours. My concern grew. Fortunately, the investigator in my office who was on call to launch on the next significant accident was Matt Rigsby, arguably the most knowledgeable helicopter safety expert in the FAA. As a former investigator for Bell Helicopters and aerospace engineer at the FAA’s Rotorcraft Directorate, Matt is well-known in the helicopter community. He booked a flight to Knoxville, rented a car, drove about an hour to the crash site and met up with two senior NTSB investigators (see graphic 7).

The investigators identified the initial tree strike about 400 feet south of the main wreckage on top of a 1,100-foot-high ridge. Pieces of Plexiglas and a section of the front-left skid tube were found near the tree strike. The debris path continued from the top of the ridge to the bottom, where the main wreckage was found, mostly consumed by a post-crash fire. In his nightly update, Matt remarked that the damage to the main and tail rotor blades indicated low rotational energy consistent with unpowered ground impact damage.

Fuel Pump
The fuel pump was removed from the engine accessory gearbox and disassembled (see graphic 8 previous page). Removal of the drive shaft revealed that its small splines, which are normally mated to the internal splines of the fuel pump drive gear, exhibited evidence of severe damage and worn spline teeth. The drive shaft spacer exhibited thermal distress and indentations consistent with contact with the internal splines of the drive gear (see graphics 9 and 10). Disassembly of the engine fuel pump revealed anomalous and accelerated spline wear that was severe enough to prevent the fuel pump from delivering fuel to the engine, resulting in a total loss of engine power.

The illustrated parts list for the fuel pump’s component maintenance manual (CMM) allowed for 11 different sizes of drive shaft spacers. According to the CMM, measurements taken during assembly of the pump’s drive shaft are used to select the proper spacer thickness. The spacer installed on the accident pump drive shaft was about 0.240 inches thick (see graphic 10). However, the original 1985 build record from the pump manufacturer indicated a spacer with only half that thickness was installed.
Review of maintenance logs revealed that the helicopter and engine had accumulated 22,562 hours and 8,550 hours respectively at the time of the accident. The helicopter had been operated for about 40 hours since its most recent and concurrent 100-hour and annual inspections. The engine fuel pump was installed seven years prior to the accident and had accumulated 1,078 flight hours since its last overhaul at that time, which was performed at a facility in Colorado in accordance with the CMM. No anomalous findings were recorded. The overhaul interval was 4,000 hours, so, in theory, the pump should have been in good condition. What happened?
In its final report, the NTSB stated that the wear on the splines of the fuel pump drive shaft was likely accelerated due to a lack of grease. Remnant material on the splines was consistent with grease being present on the shaft at one time, but it could not be determined if it was from the last overhaul or an earlier one. Additionally, drive gear spline impressions on the drive shaft spacer were consistent with an erroneously selected spacer. The incorrectly sized spacer likely resulted in a gap between the spacer and drive gear that provided a path for grease on the splines to escape. The investigation could not determine when the incorrectly sized spacer was introduced into the fuel pump assembly.
The NTSB determined the probable cause was “an inflight loss of engine power due to a failure of the engine fuel pump, which … resulted from the absence of adequate grease…” As with the Hawaii accident that occurred two months prior, the absence of grease on a spline shaft led to a fatal accident.
Lessons Learned
As stated in a recent safety alert and video produced by the NTSB and HAI, “helicopter safety starts in the hangar.” Proper maintenance procedures and inspections are particularly critical for helicopters because of their mechanical and operational complexity. A lack of vigilance in performing maintenance tasks, or in verifying that the work was done correctly, can lead to accidents. So, what can maintenance technicians do? Here are a few suggestions:
• Carefully follow the manufacturer’s instructions and manuals when performing a task to ensure that the work is completed as specified.
• Have a qualified person, other than the person who performed the maintenance, inspect critical items that have received maintenance. Ask questions if something is unfamiliar.
• Use work cards to document maintenance steps. If none are available, consider developing them from available maintenance manuals.
• Be thorough when performing routine inspections.
• Keep yourself and your maintenance staff educated and trained. Read up on the many resources from the FAA, such as Advisory Circular AC 43-13-1B, and keep abreast of the findings from helicopter accidents.